


While doctors don’t need to know all the technical detail about how mycology tests are developed and carried out, it is very important to have an overview so that they can order the appropriate test/s for their patient and interpret the results.
- Which type of sample is required (e.g. sputum vs BAL)
- Which antifungals require TDM to be performed at trough concentrations
- Sources of false positives and false negatives
- How to adapt treatment if susceptibility testing gives an ‘intermediate’ result
Find a mycology reference laboratory

- Fungi generally show much slower growth than bacteria, so turnaround times are longer. Swabs taken from the throat, genitals or wounds can generally be identified within 5 days. Respiratory samples are generally identified within 14 days, but some unusual species require an extended incubation that takes 4 weeks. Cycloheximide may be added to prevent contamination by moulds from the air.
- Unfortunately the sensitivity of fungal cultures is relatively low with fungal samples (i.e. there are frequent false negatives). MRCM offers a high-volume culture (HVC) option that can greatly increase sensitivity (Vergidis et al, 2020).
- Fungi are incredibly diverse and have different nutritional requirements, so a mycology lab will use various types of agar with relevant additives. Different media can reveal characteristics important in identification, such as production of pigments or spores.
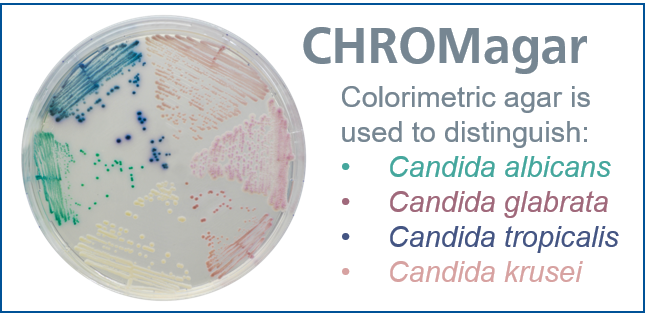
chromagar

pda
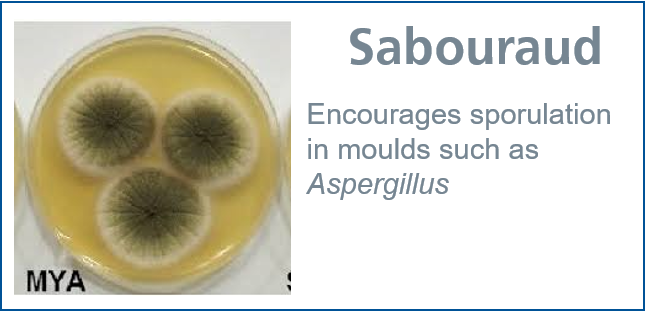
sabouraud

Most fungal infections are caused by Biosafety Level 2 organisms (e.g. Aspergillus, Candida, Pneumocystis), which can be handled by any microbiology laboratory. In very rare cases there may be a Biosafety Level 3 organism present (e.g. Histoplasma, Paracoccidioides, Talaromyces), mainly in respiratory samples from travellers returning from endemic regions.
- Find out more about Biosafety Levels at Public Health England
- Find out more about dimorphic fungi at LIFE Worldwide
BSL-3 organisms require special handling for the safety of laboratory staff and may need to be sent to the UKHSA Mycology Reference Laboratory. If in doubt, contact the laboratory before sending material and make sure samples are clearly labelled with this information.

- Simple
- Local labs routinely perform H&E staining on tissue samples. In many cases this is sufficient for identification and choosing treatment.
- Mycology reference labs use a broad selection of stains that reveal subtle structures that differ between species, which can be crucial for identification. It is sometimes necessary to use specialist agar media to grow up enough material for testing.
Histopathology stains



Microscopy stains


